
Hip resurfacing is an interesting alternative to standard hip replacement for young male patients that want to return to high impact sports or work.
Anterior hip replacement is a minimal invasive muscle sparing technique to do a hip replacement. You will not need to observe hip precautions and many patients can return to driving and working earlier than patients undergoing a posterior approach.

Anterior Hip Replacement
“Hip Arthroplasty” or “Hip Replacement”refers to the surgical reconstruction or of the hip with a ceramic on plastic or metal on plastic artificial joint.
Direct anterior total hip arthroplasty or replacement is a minimally invasive hip replacement performed to replace the total hip joint without cutting through any muscles. It is also referred to as muscle sparing surgery because no muscles are cut enabling a quicker return to normal activity and preserving the overall stability of the hip joint.
Traditionally with total hip replacement, the surgeon makes the hip incision laterally, on the side of the hip, or posteriorly, at the back of the hip. Both approaches involve cutting major muscles to access the hip joint. With the direct anterior approach, the incision is made in front of the hip enabling the surgeon to access the joint without cutting though any muscles.
Indications
Hip replacement is indicated in patients with arthritis of the hip joint.
Arthritis is a condition in which the articular cartilage that covers the joint surface is damaged or worn out causing pain and inflammation. Some of the causes of arthritis include:
- Advancing age
- Congenital or developmental hip diseases
- Obesity
- Previous history of hip injury or fracture
- Increased stress on hip because of overuse
- Femoroacetabular Impingement
Symptoms
Patients with arthritis may have a thinner articular cartilage lining, a narrowed joint space, presence of bone spurs or excessive bone growth around the edges of the hip joint. Because of all these factors arthritis patients can experience pain, stiffness, and restricted movements. This impacts their ability to walk and climb stairs. As the joint gets stiffer many patients are unable to put on their shoes and sock. Often the pain is referred to the knee and it is not uncommon to have more knee than hip pain. In the final stages of the disease patients will often wake up at night from the pain or will develop back pain because the stiff hip puts additional strain on the back.
Diagnosis
After discussing your symptoms Dr. Boettner and his team will carefully exam your hip to identify any limitations of its movement from the arthritis. While an x-ray is very helpful in evaluating the overall extend of arthritis the clinical symptoms and the degree of stiffness are often more important for the decision to move on with a hip replacement.
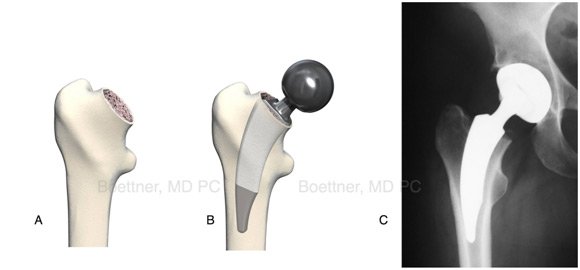
Implants:
We use special implants for anterior surgery. Usually they are shorted and curved which makes it easier to insert them into the femur from the front. Some modifications are required to insert straight stems or use cemented fixation.
Procedure
Direct anterior total hip replacement surgery involves the following steps:
- Dr. Boettner performs the surgery under regional anesthesia, called spinal anesthesia, an injection in the back that numbs the legs.
- You will you will be positioned on a special operating table (Hana® table) that enables Dr. Boettner to perform the surgery from the front of the hip and to improve access to the femur during the surgery. Usually the incision is 3-4 inches long. Dr. Boettner uses fluoroscopic imaging during the procedure to ensure accuracy of component positioning and to minimize leg length inequality.

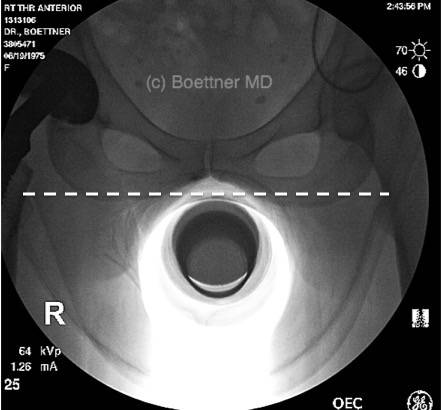
Using an image intensifier allows Dr. Boettner to accurately position the cup. An excellent cup position is important to optimize range of motion, decrease the risk of dislocation and minimize plastic wear.
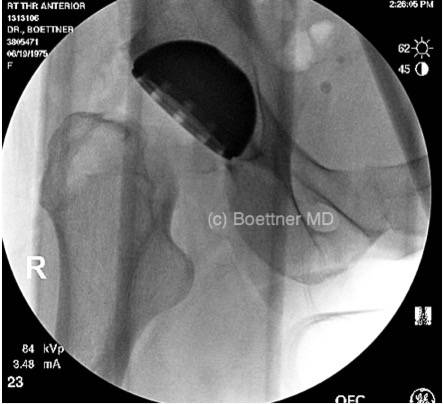
Using the C-arm x-ray Dr. Boettner is also able to judge how much anteversion the cup has, which is crucial for the overall stability of the new hip.
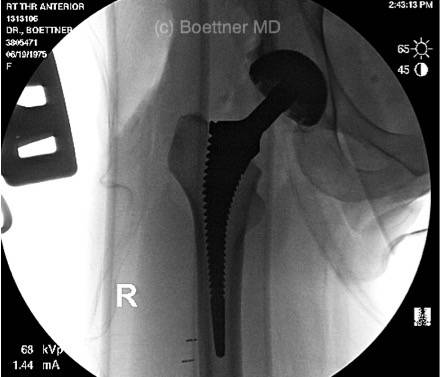
X-ray is also used to verify the stem position in the femur. This makes sure the appropriate size of the femur is choosen.
The x-ray also allows Dr. Boettner to accurately check your leg lengths. This minimizes the risk of lengthening your leg during the procedure.

With all implants in place a final check is performed to make sure everything is perfect.
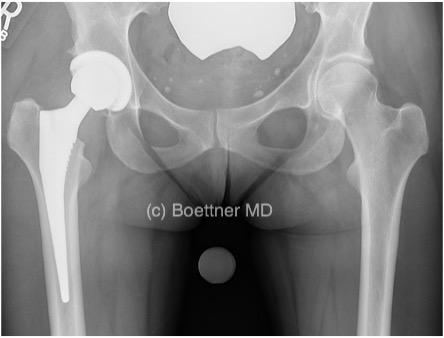
The final image shows a well positioned total hip. The use of intraoperative imaging makes it easier for the surgeon to position your hip and make sure your leg length is restored. This does directly affect your postoperative function and overall satisfaction with the procedure. The incision is closed with intracutaneous stitches and you can shower when you get home.
Post-operative care
After traditional hip replacement surgery, you would be instructed to follow hip precautions to prevent your new hip from dislocating. These guidelines are very restrictive and include no bending or flexing the hip past 90 degrees, no crossing of legs, use a pillow between the legs when sleeping, and use an elevated toilet seat.
With the anterior approach you will not have to follow standard hip precautions.
Dr. Boettner will however give you instructions to be followed at home for a faster recovery. These include:
- Take medications as prescribed to relieve pain and prevent a blood clot.
- Participate in physical therapy to restore hip function and strength
- Eat a healthy diet and do not smoke to facilitate healing and promote a faster recovery.
Contact your doctor if you observe drainage from the incision or a fever. You can drive and return once you are comfortable. Usually patients are able to drive by 2 weeks and return to work depending on the job between 7 and 28 days after surgery.
Out of state patients:
You can fly home after you are discharge from the hospital. Most patients that are operated on Friday will fly back Tuesday. Please discuss this with Dr. Boettner. He will give you stronger blood clot prophylaxis on the day you fly and give you special instructions for getting through the airport. Some patients decide to stay in New York for 2 weeks to do their rehab and have the final check up with Dr. Boettner before they leave.
Risks and complications
All surgeries carry an element of risk whether it is related to the anesthesia or the procedure itself. Risks and complications are rare but can occur. Below is a list of complications that can occur following anterior hip replacement procedure:
- Infection at the incision site or in the joint space:this can require further surgery including removal of the hip and treatment with antibiotics
- Fracture:the risk of fracture is slightly increased with an anterior approach since the exposure of the femur is not as straight forward as with a postieror approach, also not all implants can be used through an anterior approach and cemented component position requires adjustments in the incision length and might require additional muscle releases
- Nerve damage:large nerve’s can be damaged resulting in weakness and numbness. A skin nerve on the side of the hip (the lateral femoral cutaneous nerve) is very close to the incision and its injury can result in numbness on the side of the thigh
- Hemarthrosis-excess bleeding into the joint after the surgery and blood transfusion: Dr. Boettner does not recommend to routinely donate blood since the risk of a transfusion is low
- Deep vein thrombosis (blood clot) or pulmonary emboli a potentially very serious complication: we mobilize you early and put you on a blood thinner to reduce the risk. Please tell us if you had a blood clot in the past or have a bleeding disorder
- Dislocation: dislocations are rare after anterior surgery, but that does not mean that the risk is zero
- Leg length inequality: x-ray imaging is not always 100% accurate or sometimes the surgeon might decide to increase the leg length to provide better stability or might not be able to think the choosen implant as far into the canal as he hoped for.
- Loosening and wear of the implants. We today believe that implants can last your life however probably 2-5% of patient need another surgery within 10 years and maybe around 10% by 20 years.
- Major risks: any surgery has the risk of serious medical complication (like a heart attack, stroke, major bleeding) that can be life threatening. We will check all our patients carefully before the surgery, and while serious complications are extremely rare they can occur even in healthy patients.

 Anterior Hip Replacement
Anterior Hip Replacement Hip Resurfacing
Hip Resurfacing Hip Arthroscopy
Hip Arthroscopy Bearing Surface Options
Bearing Surface Options Ask the Doctor
Ask the Doctor Patient Portal
Patient Portal Patient Education
Patient Education Am I a Candidate
Am I a Candidate Patient Form
Patient Form Patient Testimonials
Patient Testimonials-
 East River Professional Building 523 East 72nd Street, 7th Floor New York, NY 10021
East River Professional Building 523 East 72nd Street, 7th Floor New York, NY 10021 -
333 Earle Ovington Blvd Suite 106, Uniondale, NY 11553
-
HSS Westchester Outpatient Center, 1133 Westchester Avenue, White Plains, NY 10605
-
 Phone Number
Phone Number -
 Fax(212) 774-2286
Fax(212) 774-2286
-
 Email
Email -
 Website
Website
Home | Disclaimer | Privacy | Sitemap | Feedback | Tell a friend | Contact Us | Accessibility Statement